



Is the Crohn’s MAP Vaccine going to be preventative or curative?
Both! The Crohn’s MAP Vaccine is a modern vaccine. Modern vaccines can be used to treat infectious diseases as well as preventing them. They do so by stimulating the immune system to produce millions of anti-MAP immune cells (called T cells) which target and eliminate MAP-infected cells in the body. Extensive tests in mice, and more recently in cattle, have shown the vaccine to be a powerful, safe and long-lasting stimulant of anti-MAP immune cells with no serious adverse effects. It is highly effective against MAP infection in animals and has an excellent chance of doing the same thing for people with Crohn’s Disease. READ MORE: https://crohnsmapvaccine.com/vaccine
Can I be involved in the Vaccine trial? And when is the Vaccine likely to be available?
A phase Ia safety trial in healthy human volunteers began in March 2017 and was completed successfully. This will be followed by a Phase Ib trial, anticipated to begin in the first half of 2021. The Phase Ib trial will be a single-centre trial based at St. Thomas’s Hospital, London, UK in 20 adults with Crohn’s Disease and will last 1 year. The estimated timeline of the Vaccine manufacture and trials is shown in the Gantt Chart below (but needs updating as there have been inevitable delays due to Covid-19). The patients recruited to this trial will need to meet strict entry criteria; there are stringent regulations which we have to obey and the trial will be governed by the close scrutiny of the regulators. Regrettably we cannot invite people to take part in the trial at this time. However, the results of the trial will be analysed in real time as it proceeds. Following the demonstration of safety and efficacy, it is anticipated that the Vaccine technology would be licensed to a pharmaceutical company to make it available to all who need it through health services worldwide -as part of this, larger Phase 3 trials inviting wider participation would be expected. The manufacture and trial of the Vaccine is being funded through investment in the company HAV Vaccines Ltd (HVL) -completion of the trial according to this timescale is dependent on HVL to secure the remainder of the funding required.
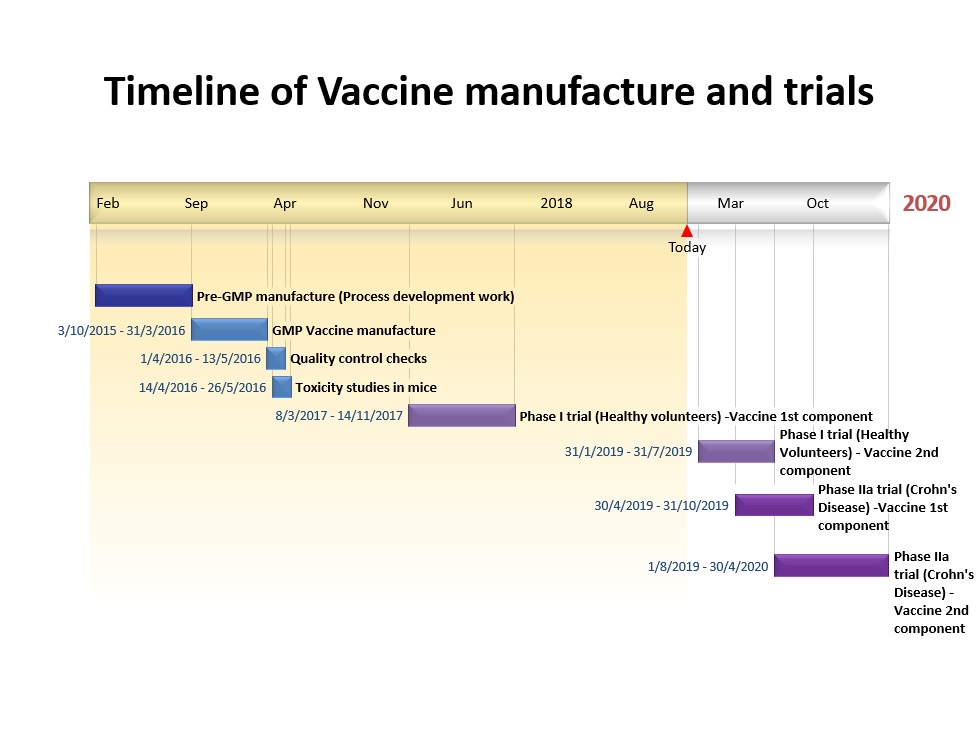
Timelines are current best estimates and are not set in stone. Delays are commonplace in research due to the unpredictable nature of organising and running trials (last updated 09.10.2019)
How will the Vaccine tie in with other treatments for Crohn’s Disease?
Some of the currently available treatments for Crohn’s Disease would be expected to potentiate the effect of the vaccine i.e. increase the response of the immune system against MAP following vaccination. These include anti-MAP antibiotics (e.g. Rifabutin, Clarithromycin and Clofazimine) and some of the conventional immunosuppressive agents (e.g. Azathioprine, 6-Mercaptopurine, Methotrexate) which have actually been shown to possess direct anti-MAP activity. The position with regard to anti-MAP vaccination in people on treatment with the anti-TNF agents Infliximab (Remicade) and Adalimumab (Humira) is not yet clear. These agents are complex immuno-modulators (i.e. they alter the way that the immune system works) and could potentially blunt responses to the vaccine, if given concurrently. But sometimes with MAP, what actually happens is the opposite of what you would first expect. Remicade and Humira work by causing the death of immune cells in the Crohn’s disease inflammatory response. Some of these cells are loaded with MAP which would probably be killed at the same time. So anti-TNF agents also have an unexpected anti-MAP action (see also FAQ 10). Ultimately, the trial and the new MAP test will give us the answers to these questions.
Will the Vaccine help Ulcerative Colitis?
‘Pure’ Ulcerative Colitis (UC) is a different disease to Crohn’s, even though many of the symptoms are similar. It is not caused by MAP but is thought to be an auto-immune disease, the trigger for which is still unknown. Crohn’s Disease is caused by MAP infection in a genetically susceptible individual. The latest diagnostic techniques detect MAP in approaching 100% of Crohn’s patients.
You can, however, get MAP superinfection in someone with UC, making the UC worse. It is also well-known that diagnostic uncertainty is a big problem in Inflammatory Bowel Disease (IBD)… so in someone mistakenly diagnosed with UC when it is actually Crohn’s disease, MAP will be the cause.
If you have UC, there are 3 ways in which the Vaccine could help:
- It is pure UC. Anti-MAP vaccination would protect against secondary MAP infection.
- It is UC but superimposed MAP infection is making it worse. Anti-MAP vaccination should improve symptoms.
- It looks like UC but it is actually Crohn’s. The vaccine is designed to fix it…and if it works in humans as it does in cattle, it should do so.
The new MAP test currently being validated is a simple, smart test which can be done on blood samples or routine gut biopsies. It is highly accurate and quantitative and will help to dispel this kind of diagnostic uncertainty in IBD.
People were talking about a Crohn’s Vaccine 10 years ago. Can you explain the project timeline? Why has it taken so long and how has funding for the project been spent?
The work towards a Crohn’s Vaccine began in 1997 and has fallen naturally into 3 stages: Vaccine development, Vaccine trial and MAP test development.
The vast majority of the money has come, and continues to come, from Crohn’s disease people and their families together with small private Trusts often with links to people affected by the disease. Without this, neither the anti-MAP vaccine nor the new MAP test would exist. Long experience has shown that conventional grant applications in our field will almost invariably be rejected. Far from being over, the fundraising and investment has to continue and intensify for a bit longer until the Crohn’s vaccine, together with its companion diagnostic, are proven by us to be safe and effective in humans. We would then envisage it being made available to Crohn’s patients in accordance with national guidelines (for example the Early Access to Medicines Scheme in the UK), while at the same time getting it entrusted to industry for assured delivery into the clinic.
So, we still have the last bit to do. But now the end is in sight. The huge generosity of very many people cannot be overstated. Similarly the fantastic work of our fundraisers starting with Nickie and Tom Colville and their family and friends whose early contributions were so pivotal. We now need our growing band of supporters all over the world to unite and help us finish this. If you would like to help, visit our fundraising page to find out more and do please get in touch.
Why has it taken so long?
Making a new treatment and prevention for a disease, particularly where a cause has not been recognised, and getting it to the people who need it does take time. Then there are inevitably setbacks along the way which cause delays and have to be overcome. For the vaccine there were three main ones.
- The first was over the period 2000-2004 when virally vectored vaccines were still in an early stage and there were problems with getting the core of the vaccine into the right vectors and with the subsequent stability of the vaccine. These were overcome particularly by the work of our collaborators at the Jenner Vaccine Institute, Oxford University.
- The second was 2007-2010 after we had successfully made and tested the vaccine in mice and needed the funding to trial it in cattle. This was overcome by a consortium, led by Dr Tim Bull, who were eventually funded in 2010 by the UK Biotechnology and Biological Sciences Research Council (BBSRC).
- The last came with the results of clinical trials of a vaccine against AIDS sponsored by the National Institutes of Health in the USA. These created uncertainty about the use of the otherwise safe and effective viral vector hAd5 -a harmless derivative of the ordinary human cold virus. Many people had pre-existing natural immunity to it. The story is most recently summarised in Science 2014; 344:49-51. We and many others working on new modern vaccines had selected hAd5 as the best-in-class priming vector and it worked safely and well in mice and even more so in cattle. However, alternatives had to be found and adapted to the vaccine vector role in humans. This took time over the period 2007-2012 but is now in place. Thanks again to the great people at the Jenner Vaccine Institute, Oxford University.
Some gastroenterologists do not think that MAP is the cause of Crohn’s disease. What arguments do they put forward AGAINST MAP as the main cause of Crohn’s?
- There just isn’t enough evidence for it.
- MAP has not been consistently detected in Crohn’s tissues. Historically, MAP has been very difficult to detect as you can’t see it under an ordinary microscopy, it is very difficult to grow it in culture and even modern techniques using PCR (testing for MAP by the presence of its DNA) have been hampered by difficulties ‘cracking open’ the tough MAP bug to release its DNA. Using careful methods, MAP has been found in 92% of CD tissues vs 26% of controls using PCR 1 Until recently, scientists have been unable to come up with a way to see MAP clearly within the tissues, but now, with the new MAP test that Prof. Hermon-Taylor has developed we are seeing it, in intricate detail, for the first time ever; so far in 100% of CD tissue samples tested (unpublished data).
- CD is not cured by ordinary anti-mycobacterial drugs. MAP is generally resistant in vivo to drugs conventionally used in the treatment of tuberculosis. Even with the correct antibiotics, MAP infections are difficult to eradicate. Treatment is prone to problems with development of antibiotic resistance by MAP and latency – a state of ‘hibernation’ which MAP (like similar organisms) can enter, in which it is very difficult to kill with drugs 2 (see also FAQ 7).
- Just because MAP is present, doesn’t mean that it causes disease. It could just be an ‘innocent bystander’, colonising the gut lining because of inflammation. If MAP was there merely due to the presence of inflammation then you would expect to find similar rates of MAP in Ulcerative Colitis as you do in CD. The fact that detection rates of MAP in ulcerative colitis are far lower than they are in Crohn’s Disease refutes this theory 3
- MAP is more likely to be a secondary pathogen; in some people MAP colonisation might contribute to the disease process but it is not actually causative. Koch’s postulates (the criteria historically required to establish a micro-organism as the cause of a disease) have been fulfilled for MAP in CD 4,7. Relman’s criteria 5 (the update to Koch’s postulates incorporating the modern molecular methods now available) have similarly been fulfilled 6,7. In addition, anti-MAP antibiotic therapy is frequently successful in inducing remission in CD (see FAQ 7)
- How can MAP be causing CD when it is present in a proportion of healthy people who do not have the disease? As with many other infections, development of disease is determined not only by the bug itself but by how the person’s immune system reacts to it. We know that development of CD in response to MAP infection requires additional ‘susceptibility factors’ (see our section on ‘MAP’ and FAQ 14). There are also many cases where a single bug can result in a spectrum of different disease states in different people. H. pylori, for example, is well-known to cause asymptomatic carrier state, mild gastritis, stomach ulcers and stomach cancer. In parallel to this, it may actually be more helpful to think of MAP infection as spectrum of increasingly hostile relationships with the human host: from an asymptomatic carrier status, through irritable bowel syndrome (where there is also evidence of MAP causation), to CD itself.
- How can CD be caused by MAP infection when immune suppression with anti-TNF drugs like Remicade and Humira, which would make tuberculosis a lot worse, can actually make CD better? Tuberculosis actually has properties which make it unique amongst the mycobacterial family. It makes more sense to compare MAP to its more typical ‘cousin’ Leprosy (caused by Mycobacterium Leprae); a disease which likewise does not worsen with when treated with anti-TNF agents 7. Plus, as explained in FAQ 10, anti-TNF agents also have significant anti-MAP action too.
- Bull T et al. Detection and verification of Mycobacterium avium subsp. paratuberculosis in fresh ileocolonic mucosal biopsy specimens from individuals with and without Crohn’s Disease. J. Clin. Microbiol. 2003; 41(7): 2915-2923
- Hermon-Taylor J. Mycobacterium avium subspecies paratuberculosis, Crohn’s Disease and the Doomsday Scenario. Gut Pathogens 2009; 1:15
- Sartor RB. Does Mycobacterium avium subspecies paratuberculosis cause Crohn’s Disease. Gut 2005; 54:896-898
- Van Kruiningen HJ et al. Experimental disease in infant goats induced by a Mycobacterium isolated from a patient with Crohn’s disease. Dig Dis Sci 1986; 31:1351-1360
- Fredericks DN, Relman DA. Sequence based identification of microbial pathogens: a reconsideration of Koch’s postulates. Clin Microbiol Rev 1996; 9(1):18-33
- Chamberlin W et al. MAP-associated Crohn’s Disease: MAP, Koch’s postulates, causality and Crohn’s Disease. Dig Liver Dis 2007; 39:792-794
- Gitlin L et al. Mycobacterium avium ss paratuberculosis-associated Diseases. Piecing the Crohn’s Puzzle Together. J Clin Gastroenterol 2012 Sep;46(8):649-655
Are any treatments for MAP currently available?
Yes there are treatments for MAP! Crohn’s Disease can be treated with anti-MAP antibiotic therapy. The protocol for this combination therapy includes Rifabutin, Clarithromycin and often a 3rd agent, Clofazimine. These are DIFFERENT antibiotics from those such as ciprofloxacin or metronidazole which mainly kill the overgrowth of other gut bacteria rather than having significant action against MAP itself.
Side effects of anti-MAP antibiotics can limit their use in some people. But in those who can take them, many will benefit from treatment and profound remissions can occur, even in those with severe disease. In some cases, major surgery has been avoided.
What is the success rate of anti-MAP triple therapy? In ordinary terms, of 5 people who can take it, 2 will get a complete remission, 2 will get a partial remission and one will not respond, probably because the MAP in that person is already resistant.
A review of the published scientific literature reveals 7 clinical trials which have investigated the effects of anti-MAP therapy in Crohn’s Disease, with clinical remission rates ranging from 44-89%1. Of these, the ‘landmark study’ is considered to be that conducted by Selby et al.2 in Australia in 2007; it is the only large randomized controlled trial and hence the most well-known. The failure of this study to show a long-term benefit of anti-MAP therapy in Crohn’s Disease is regarded by many as the ‘final nail in the coffin’ for the MAP/Crohn’s hypothesis and is a major reason for the reluctance of some Gastroenterologists to recommend this treatment to their patients. However, the trial has since been widely criticized, both in terms of the protocol used and the subsequent analysis 1,3,4, such that it cannot be relied upon as having any clinical significance. Major flaws include the following:
- Patients were not tested for MAP before entry into the trial.
- Subtherapeutic doses of all 3 antibiotics were used.
- The clofazimine capsules used failed to dissolve, thereby not releasing the active ingredient within.
- The results were not based on an intention-to-treat analysis and may have underestimated the beneficial effect of treatment 4.
Despite these flaws, the trial still demonstrated a remission rate of 66% (of 102 patients with Crohn’s Disease) at 16 weeks (p<0.02).
A fresh start has been badly needed for a long time, but there is new hope on the horizon that the true potential of this treatment may finally be revealed. In the USA, a large multi-centered randomized-controlled trial is currently underway entitled ‘Efficacy and Safety of Anti-MAP Therapy in Adult Crohn’s Disease (MAPUS)’. The anti-MAP therapy being used in this trial is a fixed-dose combination of Rifabutin, Clarithromycin and Clofazimine combined into a new 3-in-1 pill called RHB-104: http://clinicaltrials.gov/ct2/show/NCT01951326?term=crohn%27s+disease+redhill&rank=1
Are there any side effects?
Overall, anti-MAP therapy is well tolerated by the majority of patients. But as with most medicines, there are potential side effects which may be experienced by some people. Common side effects include a ‘tanned’ appearance and aching joints. More rarely, patients may experience a rash or the more serious, but reversible, condition ‘uveitis’ (inflammation of a part of the eyes) which would require treatment to be stopped. Very occasionally treatment may exacerbate disorders such as depression. Treatment should only be undertaken with close medical supervision.
Why do some people with Crohn’s not improve with anti-MAP therapy?
- A small proportion of people won’t be able to tolerate treatment.
- Mycobacterial resistance to antibiotics is well-described in the literature and becoming more common, so if you had a resistant strain of MAP already then the antibiotics would not work. It is not possible to do sensitivity studies prior to starting therapy because of the difficulty in culturing MAP.
- Prescribing problems: The preferred regime is triple therapy with Rifabutin, Clarithromycin and Clofazimine although in some people Rifabutin and Clarithromycin alone work well. Antibiotic monotherapy is well-known to lead to resistance. Correct dosing is important as opposed to that used in the trial by Selby et al.
- Inadequate duration of treatment: As with other mycobacterial infections, treatment needs to be continued for a long time (18-30 months) to ensure as far as possible that latent organisms are eliminated as well. In some people, particularly those who have not had longstanding Crohn’s disease, improvement can appear within 4-6 weeks. In others with longstanding Crohn’s disease, it can take 6 to 12 months before a real improvement occurs. In these people there is a lot of damage to the gut wall, the immune system and the delicate gut nervous system which has to be repaired.
Whilst antibiotic treatments can be a real help, they are not always a long-term solution, due to the ever-present threat of developing resistance and the ability of MAP (like other similar organisms) to go into ‘hibernation’ or latency in which state they are very difficult to kill with drugs. We need to follow the lead of our US counterparts and invest in the development of the promising anti-MAP Vaccine.
- Chamberlin W, Borody TJ, Campbell J. Primary Treatment of Crohn’s Disease: Combined antibiotics taking centre stage. Expert Rev Clin Immunol 2011; 7(6): 751-760
- Selby W, Pavli P, Crotty B et al. Two-year combination antibiotic therapy with clarithromycin, rifabutin and clofazimine for Crohn’s disease. Gastroenterology 2007; 132(7): 2313–2319
- Lipton JE, Barash DP. Flawed Australian DC trial does not end MAP controversy. Gastroenterology 2007; 133:1742
- Feller M, Huwiler K, Schoepfer A et al. Long-term antibiotic treatment for Crohn’s disease: systematic review and meta-analysis of placebo-controlled trials. Clin. Infect Dis. 2010; 50(4): 473–480
MAP Testing: can I get tested for MAP?
MAP testing is not available through hospital clinics; it is currently only done in research laboratories. No tests for MAP are yet clinically validated although with the modern methods used they are highly accurate and sensitive. This is the case worldwide, not just in the UK. The lack of a reliable MAP test that can be accessed via clinics is a major unmet medical need. Prof. Hermon-Taylor is completing the validation of a new diagnostic test for MAP at King’s College London. This is a smart, simple, highly accurate test which can be done on a blood or tissue sample. It will be automatable so that many tests can be done very quickly, using standard equipment already available to hospital labs across the world. In its final automated form, the test will take around 15 mins to run. Prof. Hermon-Taylor’s lab currently runs the manual prototype of the test on tissue samples. These can be fresh or stored samples i.e. if someone with Crohn’s has previously had surgery or a biopsy, segments of the tissue taken would be embedded in paraffin and stored in the lab at the hospital; these can be used retrospectively to test for MAP. A new blood test is also now being validated by Prof. Hermon-Taylor. Prof. Hermon-Taylor would dearly love to be in a position to offer the test to all our supporters who want it right now. Unfortunately, there are just not the resources to do this; running the test in its current form is a time-consuming process and if his time was spent running tests then no research progress would be made. We therefore need to focus our energies on completing the work –and raising the funds to enable us to do so -so that the test can be made available to everyone as soon as possible.
Johne’s Disease is easily transmitted throughout an entire herd by shedding of MAP, why does this not happen in humans? Can you catch MAP from someone with Crohn’s Disease?
Johne’s disease is an animal form of inflammatory bowel disease, known to be caused by MAP. It particularly affects domestic livestock; data from the US suggest 91% of dairy herds are infected. Not all infected animals show outward signs of disease. The poo from MAP-infected cows contains huge numbers of MAP. This poo contaminates the grass which means other grazing cows get infected. Other animals such as rabbits also eat contaminated grass; they then get infected, amplify the MAP and shed it in their pellets. Cows eat the rabbit pellets when they graze and re-acquire MAP which has cycled through another host-animal. Cycling through different species like this can make MAP more virulent, as it does with other disease-causing bacteria. Transmission between humans would not work like this under normal circumstances. People with Crohn’s have MAP in their poo too but cross-contamination and ingestion of poo on the scale seen in animals would not occur. It is also well-recognised that infections with bacteria from the Mycobacterium avium family usually result from environmental exposure rather than person-to-person transmission. So NO –it is very unlikely that you could catch MAP from someone with Crohn’s Disease.
Many people with Crohn’s Disease take immunosuppressants. If Crohn’s is caused by an infection, wouldn’t the disease get worse with immunosuppressants?
Immunosuppressants used to treat Crohn’s Disease include Azathioprine, Methotrexate and 6-Mercaptopurine as well as the newer ‘biological’ or ‘anti-TNF’ agents Infliximab (Remicade) and Adalimumab (Humira). If these were given to someone with an infection like tuberculosis, they would make the disease worse. Hence checking for latent (inactive) TB is an essential precaution before giving biological agents. So it’s not unreasonable to presume that the same would happen with immunosuppressants and MAP. But as so often with MAP, it turns out to be the opposite of what you would expect…
In the case of Azathioprine, Methotrexate and 6-Mercaptopurine, independent research by 2 groups in the USA has shown that all three of these drugs have a direct anti-MAP action1,2. They do not kill MAP but they do retard its growth and activity. Some of the benefit from these drugs is probably due to this slow anti-MAP action and is one of the reasons they take 2-3 months to work in Crohn’s disease.
TNF-alpha (tumour necrosis factor alpha) is a protein produced by cells of the immune system, to help fight infections by temporarily increasing inflammation in the affected area. The anti-TNF agents work by binding to TNF-alpha anchored on the surface of inflammatory cells involved in the Crohn’s disease inflammation. This results in the death of some of the inflammatory cells, many of which will be harbouring MAP bacteria which are likely to be killed at the same time. For this reason, treatment with anti-TNF drugs has a significant anti-MAP action too.
It is also the case that a lot of the actual damage to the gut wall in Crohn’s Disease is due to the immune dysregulation caused by MAP, which immunosuppressants help to reduce.
- Greenstein R et al. On the action of Methotrexate and 6-mercaptopurine on M. avium subspecies paratuberculosis. Plos One 2007; 2:e161
- Shin S et al. Thiopurine drugs azathioprine and 6-mercaptopurine inhibit Mycobacterium Paratuberculosis growth in vitro. Antimicrob Agents Chemother 2008; 52:418-26
- Bach H et al. Treatment of Crohn’s Disease patients with Infliximab is detrimental for the survival of Mycobacterium avium ssp. paratuberculosis within macrophages and shows a remarkable decrease in the immunogenicity of mycobacterial proteins. J Crohn’s Colitis 2012; 6:628-9
Why don’t dairy farmers and vets get Crohn’s Disease more often?
You might expect that occupations resulting in frequent exposure to MAP-infected animals, such as dairy farmers and vets, would be associated with a higher risk of Crohn’s Disease, but in fact, data from the US show that these occupations are associated with a significantly reduced death rate from Inflammatory Bowel Disease1. Children exposed to farm animals, particularly cattle, in early life also subsequently have a lower incidence of CD2, and in many countries Crohn’s Disease is more common in towns and cities than in the countryside.
The explanation of this apparent paradox lies in the fact that Mycobacterium avium subspecies paratuberculosis (MAP) can exist in (and switch between) two forms:
- The ‘extracellular’ form (i.e. adapted to live outside of other cells) has an outer ‘capsule’. It is easy to see under an ordinary light microscope because the capsule soaks up and retains a special red stain called Ziehl-Neelsen (ZN) stain, commonly used in medicine to identify Mycobacteria in particular. This form of MAP, excreted by the trillion by heavily infected animals, is not one to which humans are particularly susceptible and exposure to it is likely to confer some natural immunity against disease. It has been shown that occupational exposure to MAP is associated with raised levels of antibodies against MAP. The urban preponderance of CD is probably not that townsfolk have an increased susceptibility to CD but rather that country folk have some natural protection3.
- The ‘intracellular’ form (i.e. adapted to live inside other cells) sheds its capsule and in doing so becomes invisible to ZN staining procedures, since it is the capsule which picks up the stain. This ‘naked’ form, which is still very tough, is more virulent to humans and is the form found in people with Crohn’s disease. MAP adopts this form after being taken up into white blood cells in the animal’s bloodstream and tissues. These white blood cells containing MAP bugs then pass into the milk. After a while, MAP in the environment also gets taken up by single-celled amoeba-like organisms called ‘protists’ which again enhances virulence to humans. Humans are therefore exposed to the virulent intracellular form of MAP both via milk from infected cows and via water supplies from contaminated rivers.
As with almost everything to do with MAP, the truth is more complicated than it first appears and what actually happens turns out to be the opposite of what you would expect.
- Cucino C, Sonnenberg A: Occupational mortality from Inflammatory Bowel Disease in the United Stated 1991-1996. Am J Gastroenterol 2001; 96:1101-5
- Radon K et al. Chronische Autoimmunerkrankungen und Kontakt zu Tieren: Contact with farm animals in early life and juvenile inflammatory bowel disease: a case-control study. Pediatrics 2007; 120:354-61
- Hermon-Taylor J. Mycobacterium avium subspecies paratuberculosis, Crohn’s Disease and the Doomsday Scenario. Gut Pathogens 2009; 1:15
Why is it quite easy to detect MAP in the gut tissue of a cow with Johne’s disease, but it is difficult to detect in the gut tissue of humans with Crohn’s disease?
Again this comes down to the fact that Mycobacterium avium subspecies paratuberculosis(MAP) exists in 2 forms: with a capsule (the most common form in animals) and without a capsule (this form occurs universally in humans but can occur in some animals as well). The capsule stains bright red… so it is barn-door easy to see under an ordinary microscopy with ordinary procedures. Once MAP loses its capsule it becomes invisible; you can’t see it with ordinary staining procedures, it is very hard to get it to grow in culture in the lab and when it does grow it can take up to 18 weeks, even with the best modern methods. You can detect it by PCR i.e. by the presence of its DNA… but to do that, you have to crack open the bug to release the DNA. The form of MAP in humans is very small and very tough so standard procedures for releasing bacterial DNA don’t work; special measures are required. Research groups who haven’t taken heed of this in the past have found negative results, leading to conflicting data in the literature and clouding understanding amongst the medical community.
Is MAP present in the breast milk of mothers with Crohn’s Disease? Is MAP present in powdered infant formula? Could people be unknowingly exposing their babies to MAP and the risk of developing Crohn’s Disease in turn?
Dr Saleh Naser and colleagues reported the isolation of MAP from the breast milk from each of two mothers with Crohn’s disease in 2000. The milk of 5 other women without Crohn’s disease tested negative (1). MAP has also been detected in powdered infant formula. In the latest study (presented at the 12th International Colloquium of Paratuberculosis June 2014), scientists from the University of Wisconsin and Queen’s University, Belfast tested 68 samples of powdered Infant Formula from 18 countries, including 40 brands. 44% (30/68) tested positive for live MAP. These findings are in line with those of an earlier study by scientists from the Veterinary Research Institute, Brno, Czech Republic who found 35% (18/51) of powdered milk samples contained MAP (2). All of these findings require further validation and definitive answers to the above questions would only come from much larger clinical studies. However, these findings serve to highlight how important it is that we do not ignore the evidence pointing to MAP as the cause of Crohn’s disease. There exists a potential risk of exposure to MAP from both breast and bottle feeding which at present cannot be quantified.
- Naser SA, Schwartz D, Shafran I. Isolation of Mycobacterium avium subspecies paratuberculosis from breast milk of Crohn’s Disease patients. Am J Gastroenterol. 2000 Apr; 95(4): 1094-5
- Mycobacterium avium subsp. paratuberculosis in powdered infant milk: F57 competitive real time PCR
Is Crohn’s a genetic disease?
Yes and no. Whether someone gets Crohn’s Disease (CD) is not determined by a single gene as it is for, say, Cystic Fibrosis, but genes do play an important role. A new technology called Genome Wide Scanning (GWS) has enabled scientists to scan the whole length of a person’s DNA looking for small changes. This has been done for many different diseases and also comparing different human populations. It has provided hugely important new insights into the potential causes and mechanisms of disease. When GWS has been done in thousands of people with CD and compared with thousands of people without CD (either in themselves or their families), some small changes or ‘mutations’ within genes have been consistently found in people with CD. Although many genes are involved, some mutations appear more frequently and are more important than others. The three most important genes associated with CD (called NOD2, ATG16L1 and IRGM) all affect the capacity of immune cells to get rid of bugs which live inside cells… like MAP! These exact same genes are also found to be highly associated with susceptibility to Tuberculosis and Leprosy (other members of the ‘Mycobacteria’ family). The truth that GWS and related methods have enabled us to see is that very many infectious diseases may be more likely to happen in some individuals rather than others because of inherited susceptibilities. So whilst you don’t inherit Crohn’s Disease, you can inherit a susceptibility to the bug that is causing it.
How does MAP cause Crohn’s Disease?
Find out how MAP causes Crohn’s Disease here: https://crohnsmapvaccine.com/map
If MAP is the cause of Crohn’s Disease, why does enteral nutrition help so much in the treatment of many cases of Crohn’s?
The segments of gross inflammation are not caused by a direct head-to-head confrontation between MAP and the immune system, as in Tuberculosis. The primary enabling cause is because MAP infection which is throughout the gut, dysregulates the immune and enteric nervous systems which makes the gut ‘leaky.’ The secondary effector cause is the perturbed neuroimmune response to entry into the gut wall of microbiota and food residues from the gut lumen. Enteric feeding eliminates the allergic and other responses to the food residues as well as changing the nature of the gut microbiota. When you stop the enteric feeding the whole thing comes back because the underlying MAP infection and perturbed neuroimmune systems are still there. A more detailed answer is in this paper: http://www.gutpathogens.com/content/1/1/15 “Inflammation in CD caused by a two tier co-operative pathogenic mechanism”.
If this vaccine is a possible cure, why is it not already funded by one of the large foundations or pharmaceutical companies?
Foundations have very strict guidelines and require absolute adherence to all of them for a proposal to be considered. The strict guidelines include, geographical regions, i.e. funding only local projects. They may require relinquishing intellectual property rights, or they will only fund basic science research, or only young scientists. These guidelines are usually in the fine print, and have prevented foundations in the past from funding the vaccine. Often, they refuse to consider unsolicited requests. They will only look at invited proposals, which of course means, that they need to be aware of the project in order to extend an invitation. Pharmaceutical companies almost always wait until phases 1 and 2 are completed before they consider funding a project. This move from the lab bench to the bedside is problematic. There is a huge bottleneck of drugs ready for trial, at least 20 years’ worth but the companies consider it too risky and too expensive to fund phases 1 and 2. People in the field call it the valley of death; it is where drugs go to die. Thus, funding often drives research and not the other way around. However, we believe that research such as the vaccine, should in fact be driving the funding.